
Debunking the Continuous Progesterone Myth: Unopposed Estradiol Is the Real Concern

Lately, our inboxes have been flooded.
Women are reading things on social media that are frightening them, confusing them, and in some cases making them want to stop their progesterone.
So instead of trying to answer one DM at a time, I decided to bring two of the people I trust most in this space — Carol Petersen, RPh and Phyllis Bronson, PhD — to the table to talk it through together.
Here's a sample of what women have been asking us:
"I've heard daily progesterone may increase my risk for dementia. Is that true?"
"Should I be cycling my progesterone instead of taking it every night?"
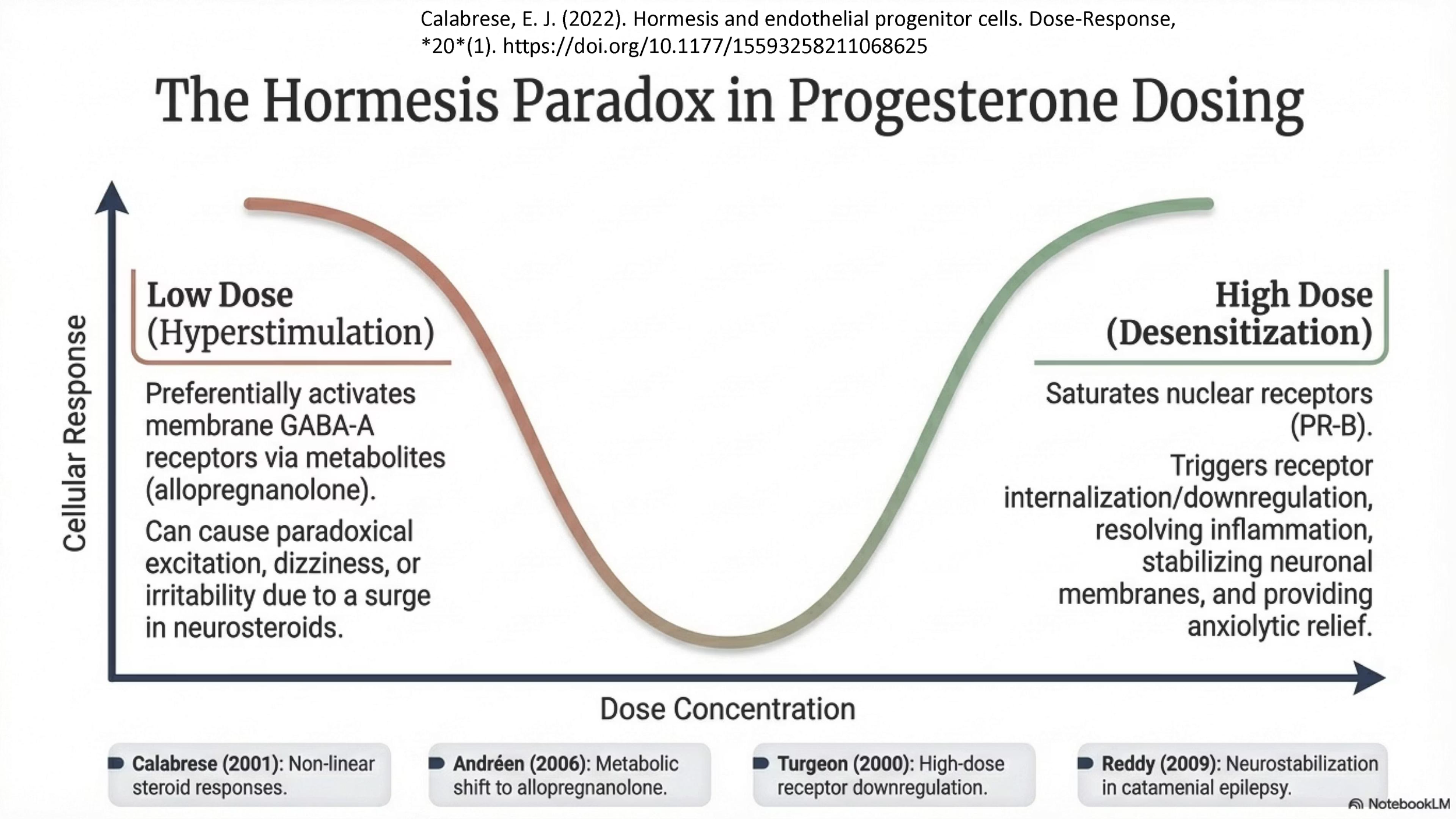
"Is oral progesterone dangerous because it acts like a benzodiazepine? If I need it to sleep, am I addicted?"
"Should I only be using vaginal progesterone?"
"Doesn't progesterone shut down my estrogen receptors everywhere, including my brain?"
"I don't make progesterone the first two weeks of my natural cycle, so why would I take it every day?"
These are good questions. They deserve real answers. And the bigger conversation underneath them, the one that often gets missed, is about what happens when estrogen is given without progesterone to balance it. Even briefly.
So in this conversation, Carol, Phyllis, and I walked through what the evidence actually says, both the research and decades of clinical experience, and how to think about all of this for your body and your life.
About Phyllis Bronson, PhD
Phyllis Bronson, Ph.D., holds a doctorate in biochemistry. Her ongoing research involves studying the biological impact of molecules on mood and emotion. Dr. Bronson works with women who have hormone-based mood disorders, utilizing her original research on human identical hormones. She lives in Aspen, Colorado, and is President of Biochemical Consulting and The Biochemical Research Foundation. Dr. Bronson is the author of Moods, Emotions, and Aging: Hormones and the Mind-Body Connection,and has authored many articles, which can be found here.
In the Aspen area? On July 27th, the Jewish Community Center in Aspen will be hosting The Great Hormone Conversation with Phyllis and Dr. Alan Altman. For more info or tickets,click here.
About Carol Petersen, RPh, CNP
Carol Petersen is an accomplished compounding pharmacist with decades of experience helping patients improve their quality of life through bioidentical hormone replacement therapy. She graduated from the University of Wisconsin School of Pharmacy and is a Certified Nutritional Practitioner. Her passion for optimizing health and commitment to compounding is evident in her involvement with organizations including the International College of Integrated Medicine and the American College of Apothecaries, the Academy of Anti-Aging Medicine (A4M), American Pharmacists Association and the Alliance for Pharmacy Compounding.
She was also the founder and first chair for the Compounding Special Interest Group with the American Pharmacists Association. She chairs the Integrated Medicine Consortium, an umbrella group for complementary medicine organizations. She cohosts a radio program, “Take Charge of Your Health,” in the greater New York area. She is on the Medical Advisory Boards for the Centre for Menstrual Cycle and Ovulation Research (CeMCOR.ca) and the Institute for Bioidentical Medicine (IOBIM.org). She also writes and edits for A4M’s website www.worldhealth.net and is a co-producer of “Immortality Now” podcasts. Carol offers personal consultations at www.thewellnessbydesignproject.com.
Video Timestamps
[00:00] Opening & Why This Webinar Now
[00:30] Backstory: ~4 months of panic messages from women on social media about progesterone
[02:25] Why misinformation from influencer-doctors is dangerous; Institute of Bioidentical Medicine grand rounds
[04:19] Dr. Katarina Dalton: Dosing, and What's Been Lost
[05:41] Why serum/urine/saliva testing only shows one compartment (you miss the full picture)
[06:38] Women are frightened by the hormone content online, especially about progesterone
[07:56] Misconceptions regarding transdermal progesterone
[10:31] Allopregnanolone & the GABA-A receptor: Taking oral progesterone does not mean that you have a benzodiazepine addiction (there is no addiction mechanism)
[13:22] Why do some women have a strong response to progesterone? Detox pathway issues may explain individual sensitivity
[17:20] Debunking the myth that continuous progesterone is dangerous
[18:55] Core myth restated: progesterone does not globally downregulate estrogen. We also talk about progesterone and histamine.
[20:57] Progesterone is made every day, not just in the luteal phase
[22:04] Should postmenopausal women cycle their progesterone doses?
[25:15] Differences between progesterone (allopregnanolone) signaling at the GABA receptor and benzodiazepines signaling at the GABA receptor.
[30:00] Carol's progesterone-inversion slide — If you think you're progesterone intolerant, 90%+ of the time you're under-dosed
[35:00] Estrogen has its own metabolic pathways — progesterone doesn't override them and actually enhances estrogen receptors
[41:59] Progesterone is measurable in the follicular phase too (just lower than luteal) — comes from adrenals and ovary; there's no progesterone in the follicular phase" is 100% false
[46:00] Debunking the myth that continuous progesterone increases the risk for dementia
[47:56] Without anti-proliferative hormones (progesterone, estriol), even 3 days off raises immunological/cancer risk in vulnerable women
[55:00] Most hormone testing doesn't tell you much — symptoms are key; Dutch test critique — sound and fury signifying mostly nothing; 24-hour urine testing is an exception
[58:00] Aging well requires consistent hormone support even without ovarian cycling
[1:00:39] Prior's osteoporosis research: oral micronized progesterone 300 mg daily; build-up/break-down bone rhythm
[1:02:50] Prasterone (vaginal DHEA) — targets androgen receptors in the vulva (where pain originates)
[1:05:21] Urinary dribbling on jump/laugh = compromised tissue integrity, testosterone-dependent; untreated urinary incontinence → nursing home pipeline (anticholinergics → falls → hip fractures)
[1:09:00] Rising FSH may be the "aging switch"
[1:12:00] Progesterone lowers IL-1β and MAPK — major anti-inflammatory pathways
[1:13:50] Meningioma: contradictory literature; Phyllis would avoid progesterone, lean to a little testosterone or Bi-est; cancer is complicated
[1:15:00] The British Menopause Society "Ratio" Myth - Progesterone dose should be proportionate to estrogen — way off base
[1:19:00] Question about progesterone and breast cancer; Progesterone is an mTOR inhibitor and COX-2 inhibitor — should be used routinely
[1:24:00] 5α-reductase converts testosterone → DHT and progesterone → allopregnanolone; women + men often get testosterone without enough progesterone to balance; Symptoms of imbalance: irritability, sleep problems, headaches, "being a bully"
For more information on this topic, see our other webinars:
Missing the Mark on Progesterone: What Most Menopause Doctors Get Wrong
Disclaimer: This article is for educational and informational purposes only and is not intended to replace personalized medical advice or individualized care. It is meant to help you understand your physiology, explore evidence-based options, and make informed choices about your health and wellness. Healthcare should be a partnership, not a permission slip, and proactive care is just as essential as treatment. Use this information to engage in open, collaborative discussions with your provider or to make empowered decisions that align with your own values, goals, and comfort level. You are the ultimate authority on your body.