
What If Estrogen Isn’t the Enemy in BRCA?

Published: July 6, 2026
Most women with a BRCA gene variation have been told some version of the same story:
“Your hormones are dangerous, your ovaries are a ticking time bomb, and the safest path is to take them out early and stay away from estrogen for the rest of your life.”
I understand why that story exists. The cancer risk is real. The decisions women have to make in their 30s and 40s are heavy (to say the least).
But the more I read the actual science, the harder it is to hold that story without asking some more questions. Because the same estrogen women are told to fear may also be one of the things their cells use to fix themselves, and to keep their energy systems running.
What BRCA Actually Is
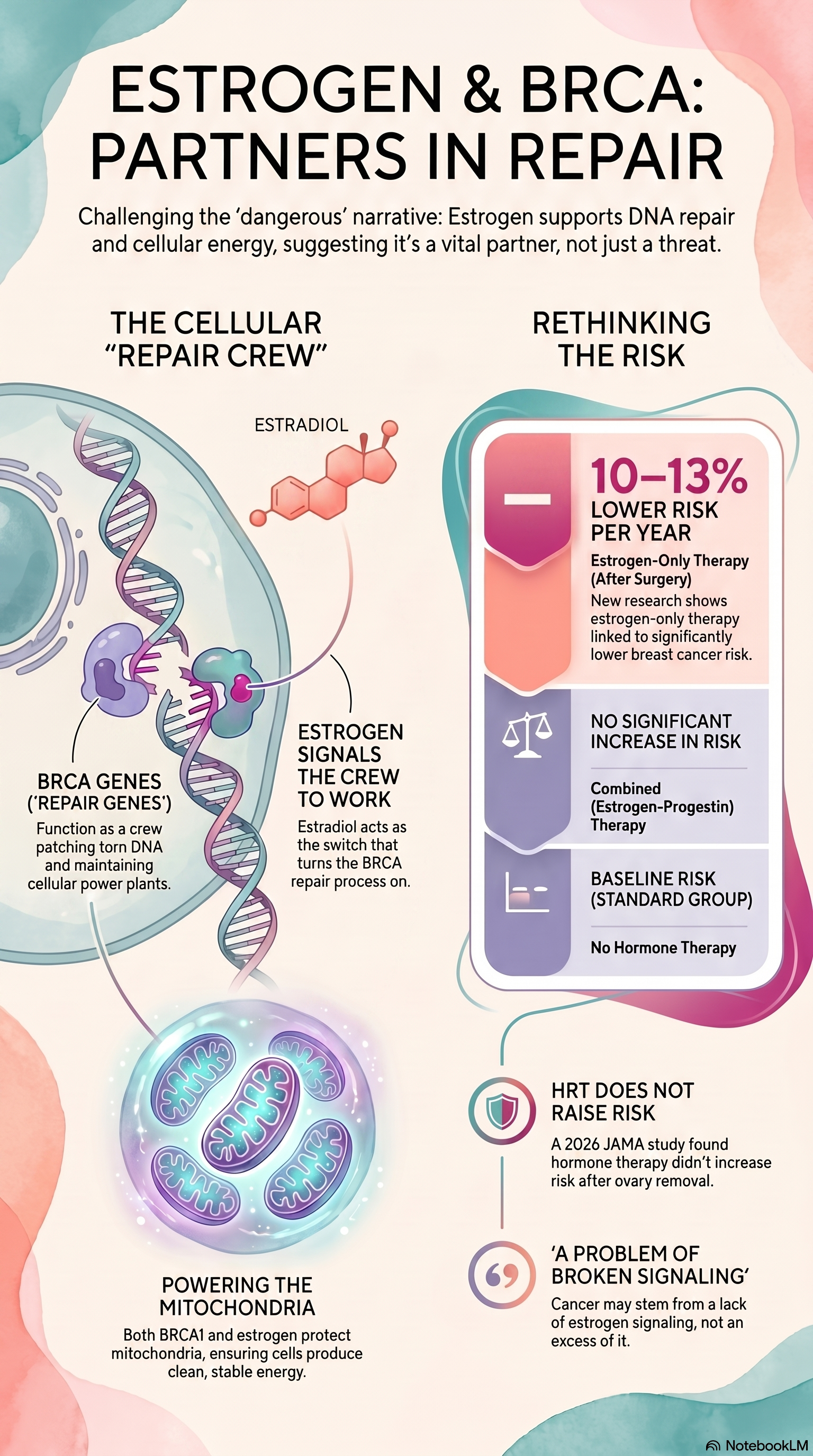
BRCA1 and BRCA2 are genes. Every woman has them. They are not “cancer genes.” They are “repair genes.” Their job is to fix broken DNA inside your cells.
Think of your cell as a small factory. The instruction manual (your DNA) is located in the factory’s office. The power plants (your mitochondria) are in the factory, helping keep it humming along. A repair crew runs back and forth between them, patching torn pages of the DNA instruction manual and keeping the power plants in good working order.
BRCA1 and BRCA2 are part of that repair crew. When the crew is working well, torn pages in the DNA manual get patched, power plants run clean, and the factory hums. When the crew is short a worker or uses a broken tool, mistakes pile up in the DNA instruction manual, and in the power plants (mitochondria).
A BRCA gene variant means the repair crew isn’t working quite as well as it should.
The Part Most Women Are Never Told: Estrogen Helps Run the Crew
Your cells don’t repair DNA on their own. They need signals. They need the right helpers in the right place at the right time. And one of the helpers that turns the BRCA repair crew on is estradiol, the main estrogen your ovaries make.
A growing body of mainstream cancer biology shows that estrogen and BRCA are partners. Estrogen helps switch the BRCA repair crew on. BRCA, in turn, helps the cell respond to estrogen in a healthy way. Take one away and the other one struggles [1, 2, 3].
When researchers take estrogen away from cells in the lab, the activity of BRCA1, BRCA2, and other repair genes drops. Add the estrogen back, and the repair genes wake up again [3]. That is not a fringe finding. That is published in mainstream cell biology journals.
The Mitochondrial Piece: Where the Whole Story Gets Bigger
Now here is where it gets really interesting, and where I think most BRCA conversations stop too early.
DNA repair is not the only job of the BRCA genes. BRCA1 also helps maintain the mitochondria, the tiny powerhouses that produce almost all of your cell’s energy. BRCA1 helps the cell keep the power plants in good shape, fuse them when they need help, split them apart when one is damaged, and clear out the damaged ones before they cause trouble [4].
When BRCA1 isn’t working well, the power plants struggle too. They don’t make energy as cleanly. They build up damage. The cell can’t clear out the damage. Energy production drops. The cell starts looking for shortcuts to keep itself alive, and one of those shortcuts is a fermentation-style metabolism that researchers like Dr. Thomas Seyfried have spent decades linking to cancer itself.
This is the metabolic theory of cancer, in its simplest form. Cancer is not just a gene problem. It is also a problem with the power plant.
When the energy system in a cell breaks down, the cell stops behaving normally. It loses the signals that tell it when to grow, when to stop, and when to die. And without enough energy, it cannot run the repair crew that would have caught early DNA damage in the first place.
So a BRCA gene change is not just “DNA repair isn’t quite right.”
It is closer to: “The office is short-staffed, AND the power plants are running dirty, AND the clean-up crew is behind on its rounds.” The damage in the DNA manual accumulates as the energy supply drops. It is a mess, and the mess feeds itself.
This is why the next piece matters so much.
Estrogen Helps Run the Power Plants Too
Estradiol not only supports the BRCA repair crew. It also supports the mitochondria directly.
Estrogen helps cells make new mitochondria. It helps the power plants assemble correctly. It boosts the amount of clean energy (ATP) they can produce. It calms the damaging exhaust fumes (reactive oxygen species) that mitochondria put out when they are stressed. And it helps the cell clean out broken power plants before they cause harm [5, 6].
In other words, estrogen is one of the body’s main signals that help keep the energy system healthy.
Now layer that onto a BRCA gene variation. The repair crew is already short-handed. The power plants are already struggling. Then estrogen, the signal that helps both the repair crew AND the power plants, is taken out of the picture, either by surgical menopause or by long-term hormone blockade.
You can see why some researchers are starting to ask whether the standard approach may be hitting the same broken system twice. Hungarian pathologist Dr. Zsuzsanna Suba has spent more than a decade arguing exactly that. She believes BRCA-related breast cancer is not a problem of too much estrogen. She believes it is a problem of broken estrogen signaling, and that the standard response of cutting estrogen off may deepen the very problem that created the risk in the first place [7, 8].
Her conclusion is not mainstream. But the biology she is pointing to is.
So, Why Are Women Told to Avoid Hormones?
Removing the ovaries (the medical word is risk-reducing bilateral oophorectomy, or rrBSO) does lower ovarian cancer risk in women with a BRCA gene variation. That part is real. Ovarian cancer is hard to catch early and hard to treat. For many women, this surgery is a serious survival tool.
And yet…..
When the ovaries come out before natural menopause, estrogen crashes overnight. The standard response has been: “That’s okay, just don’t replace it. Estrogen feeds cancer.”
But what if the body’s own estrogen isn’t the problem? What if the body needs it to keep the repair crew working AND the power plants running?
This is the question women in my community have been quietly asking for years. And now there is new evidence that says the question is worth asking out loud.
What the New JAMA Study Found
In April 2026, JAMA Network Open published a study from three medical centers in Israel. The researchers followed 919 women with a BRCA1 or BRCA2 gene change who had their ovaries removed between 2000 and 2024. They watched these women for an average of almost 9 years to see who developed breast cancer and who did not [9].
Here is what they found.
Hormone therapy after ovary removal did not raise breast cancer risk. Not for combined estrogen-progestin therapy. Not for estrogen-only therapy. The rates were essentially the same as those of the women who took nothing [9].
Estrogen-only hormone therapy was linked to lower breast cancer risk, about 10% lower for each year of use across the whole group, and 13% lower for each year of use in women with BRCA1 changes specifically [9].
Read that again. In a group of women carrying the gene change most strongly tied to breast cancer, taking estrogen after surgery was tied to less breast cancer, not more.
This is not a one-off finding. It lines up with an earlier study by Kotsopoulos and colleagues that followed 872 women with BRCA1 changes and found the same pattern: estrogen-containing hormone therapy after ovary removal was linked to about an 8% lower risk per year of use [10].
Two large studies. Same direction. In the population of women who are most often told to avoid estrogen forever.
Holding the Whole Picture
The simple message many BRCA carriers receive, that “estrogen is dangerous, avoid it for life,” is not supported by the best current evidence. Estrogen-only hormone therapy after risk-reducing ovary removal does not appear to raise breast cancer risk and may lower it.
That changes the conversation.
It means a woman in her late 30s carrying a BRCA1 change, facing the loss of her ovaries 15 years before nature would have taken them, does not have to choose between cancer prevention and the steep costs of early surgical menopause. Those costs are not small. Without hormone replacement, early loss of the ovaries is linked to higher rates of heart disease, stroke, bone loss, cognitive decline, and overall death from any cause [11].
Women deserve to know all of that. They deserve a real conversation about benefits, risks, alternatives, and the risks of not using hormones. Not a blanket “no.”
What I Hope You Take From This
If you are a woman carrying a BRCA gene variation, I am not telling you what to do. That is not my job. Your plan belongs to you, your body, your history, your values, and your clinician.
What I am saying is this. The science underneath your plan is still being written. The story that estrogen is simply a cancer driver is inaccurate. In healthy tissue, estrogen helps your cells fix their own DNA and keep their power plants running, and the BRCA repair crew is one of the teams it supports.
That is worth knowing before you agree to any medical treatments. That is worth bringing to your next appointment.
References
1. Rajan, A., et al. (2021). Deregulated estrogen receptor signaling and DNA damage response in breast tumorigenesis. Biochimica et Biophysica Acta (BBA) - Reviews on Cancer, 1875(1), 188482. https://doi.org/10.1016/j.bbcan.2020.188482
2. Yedidia-Aryeh, L., & Goldberg, M. (2022). The interplay between the cellular response to DNA double-strand breaks and estrogen. Cells, 11(19), 3097. https://doi.org/10.3390/cells11193097
3. Zach, L., et al. (2022). Estrogen and DNA damage modulate mRNA levels of genes involved in homologous recombination repair in estrogen-deprived cells. Journal of Translational Genetics and Genomics, 6, 266–280. https://doi.org/10.20517/jtgg.2021.58
4. Chen, Q., et al. (2020). BRCA1 deficiency impairs mitophagy and promotes inflammasome activation and mammary tumor metastasis. Advanced Science, 7(6), 1903616. https://doi.org/10.1002/advs.201903616
5. Klinge, C. M. (2008). Estrogenic control of mitochondrial function and biogenesis. Journal of Cellular Biochemistry, 105(6), 1342–1351. https://doi.org/10.1002/jcb.21936
6. Huang, X., et al. (2025). The role of estrogen in mitochondrial disease. Cellular and Molecular Neurobiology, 45(1), 68. https://doi.org/10.1007/s10571-025-01592-8
7. Suba, Z. (2015). DNA stabilization by the upregulation of estrogen signaling in BRCA gene mutation carriers. Drug Design, Development and Therapy, 9, 2663–2675. https://doi.org/10.2147/DDDT.S84437
8. Suba, Z. (2023). Rosetta stone for cancer cure: Comparison of the anticancer capacity of endogenous estrogens, synthetic estrogens and antiestrogens. Oncology Reviews, 17, 10708. https://pmc.ncbi.nlm.nih.gov/articles/PMC10154579/
9. Regev-Sadeh, S., et al. (2026). Hormone therapy after oophorectomy and breast cancer risk in women with BRCA pathogenic variant. JAMA Network Open, 9(4), e265648. https://doi.org/10.1001/jamanetworkopen.2026.5648
10. Kotsopoulos, J., et al. (2018). Hormone replacement therapy after oophorectomy and breast cancer risk among BRCA1 mutation carriers. JAMA Oncology, 4(8), 1059–1065. https://doi.org/10.1001/jamaoncol.2018.0211
11. Faubion, S. S., et al. (2015). Long-term health consequences of premature or early menopause and considerations for management. Climacteric, 18(4), 483–491. https://doi.org/10.3109/13697137.2015.1020484
For more information on this topic, see my other articles:
Hormones & Breast Cancer: What’s Fact, What’s Fiction?
The History of Breast Cancer Treatments and the Misguided War on Estrogen
The Truth About Estrogen, Breast Cancer, and Hormone Therapy: What the Latest Research Reveals
Check out the Breast Cancer Series in the Balance App
Disclaimer: This article is for educational and informational purposes only and is not intended to replace personalized medical advice or individualized care. It is meant to help you understand your physiology, explore evidence-based options, and make informed choices about your health and wellness. Healthcare should be a partnership, not a permission slip, and proactive care is just as essential as treatment. Use this information to engage in open, collaborative discussions with your provider or to make empowered decisions that align with your own values, goals, and comfort level. You are the ultimate authority on your body.