
Why the Testosterone Blood Test Is Not Telling You What You Think It Is

By: Jill Chmielewski, May 24, 2026
If you have ever had your testosterone checked and been told the number was “normal,” or “too high,” or “out of range,” there is something important you were probably not told.
The blood test is not measuring what most women think it is measuring.
It measures one slice of testosterone. A small one. And the lab range printed next to that number was built for a different purpose than guiding hormone treatment. Once you understand what the test actually shows, the whole conversation about dosing, safety, and “normal” levels changes.
Let’s walk through it carefully.
Where Testosterone Comes From in a Woman’s Body
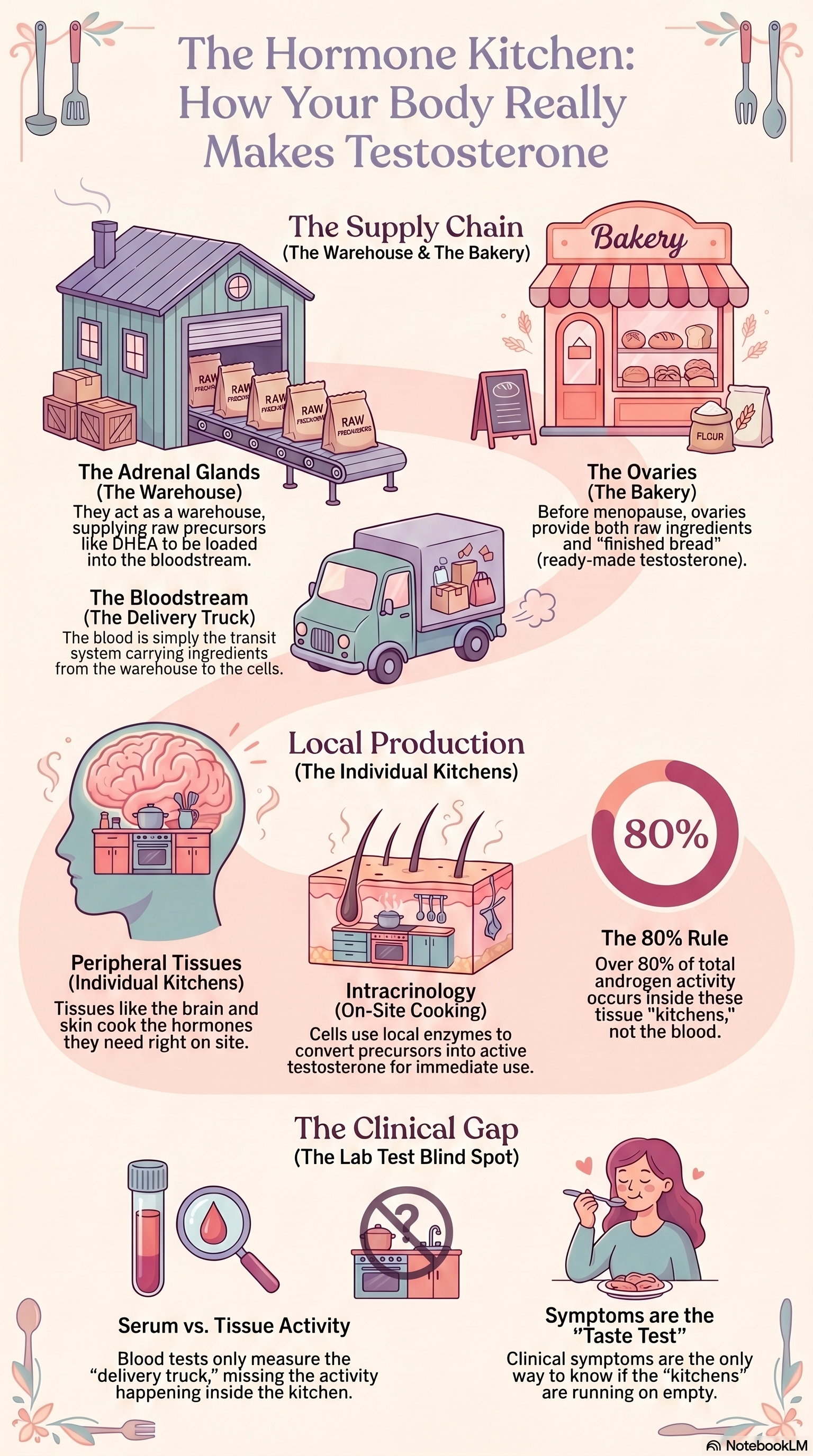
A woman’s body makes testosterone in three places [1, 2]:
The ovaries make a small, steady amount across the reproductive years.
The adrenal glands (sitting on top of your kidneys) make raw materials.
The tissues themselves — the breast, the brain, the bone, the vagina, the skin — take those raw materials and make testosterone right inside the cell.
That third one is the part most women have never heard of. It has a name: intracrinology. The Canadian scientist Dr. Fernand Labrie spent his career describing it [1, 2].
Here is the short version.
The ovaries and adrenals do not just deliver finished testosterone to the bloodstream. They deliver raw ingredients — mostly a hormone called DHEA, along with DHEA-S and androstenedione. Each tissue then picks up those ingredients and produces its own testosterone (and estradiol) right inside the cell, where it is used and then broken down on the spot [1, 2, 3].
Think of the ovaries and adrenal glands as warehouses for the raw ingredients.
Think of the bloodstream as the grocery delivery truck, carrying both already-made testosterone from the ovaries, along with the adrenal precursors, DHEA, DHEA-S, and adrostenedione to the cells for use.
Think of the tissues (brain cells, bone cells, breast cells, muscle cells, etc.) as their own little kitchens. The truck does not cook the meal. It delivers the raw ingredients so that the cell's organelles can produce the right amount of hormones the cell needs.
How testosterone is made
What the Blood Test Actually Measures
The blood test measures the testosterone on the delivery truck. It does not measure what the kitchens are actually cooking.
In women, the testosterone in the blood reflects only a small slice of the total testosterone activity in the body. Most of the bioactive testosterone, the testosterone that is actually doing the work, is made and used inside the cells, from those adrenal ingredients [1, 2, 3].
In Dr. Glaser’s most recent paper, she puts numbers on this. In postmenopausal women, more than 80% of androgen activity in the body comes from adrenal building blocks converted inside the tissues [3]. Only a small slice arrives through the blood. She also notes that serum testosterone “shows no correlation” with the body’s true androgen output once you measure the breakdown products that come from inside the tissues [3].
In plain language, the blood number cannot tell you what is happening inside the cells.
What About the Ovarian Testosterone?
The ovaries do make testosterone directly, not just precursors. Special cells in the ovaries (called theca and stromal cells) make testosterone the same way men’s testicles do — from cholesterol [4]. So the ovaries are not the same as the adrenals. They contribute a real, finished hormone to the bloodstream.
But here is what happens with age:
By the time a woman reaches menopause, her ovarian testosterone output has dropped by roughly half [4, 5].
Her DHEA, the main adrenal hormone, has dropped by about 60% by menopause and by 70–95% by older age [3, 6].
Androstenedione, another adrenal ingredient, falls by about 50% between ages 40 and 70 [3].
So both streams — the ovarian one and the adrenal one — are slowing down at the same time. And here is the bigger story. More than 80% of a postmenopausal woman’s androgen activity is made inside her tissues from those adrenal ingredients [3]. So the adrenal decline matters more than most people realize.
This is why so many women feel a shift in their 40s before their periods even stop. Your ovaries are not the only thing changing. Your adrenals are too. And the tissues that depend on both are getting less of what they need.
So Where Is the Testosterone in My Blood Coming From?
In a premenopausal woman, the blood testosterone is a mix:
About half comes directly from the ovaries.
About half is converted from adrenal precursors floating in the bloodstream [4, 5].
In a postmenopausal woman who still has her ovaries, the picture changes:
The ovaries still make some testosterone, but much less than before [4, 5].
The adrenal contribution to what shows up in the blood is also smaller because the adrenals produce fewer precursors [3, 6].
The largest source of androgen activity is in the cells of the breast, brain, bone, and vagina. That part does not show up in the blood at all [1, 2, 3].
So the blood test is measuring a smaller and smaller fraction of the actual hormone store as a woman ages. The number can look “fine” while the tissues are running on empty.
Why Dr. Glaser Will Not Dose by the Blood Number
Dr. Rebecca Glaser has been very direct about this. She does not titrate testosterone treatment by chasing a target blood level [3, 7]. She titrates based on symptoms and side effects. Her reasons, in her own words from her 2026 paper:
A single testosterone measurement is “inherently unreliable as a sole guide to therapeutic adequacy” [3].
Restoring tissue-level function in aging women “frequently necessitates steady-state serum T levels above conventional norms to offset lost adrenal contribution” [3].
In her published cohort of women on testosterone pellets, mean serum testosterone at four weeks was about 299 ng/dL. That is four to six times above the usual female reference range. She saw symptom relief and no clinically significant androgen excess [3, 7].
In other words, she is replacing not just the lost ovarian testosterone, but the lost adrenal contribution to every tissue in the body. To do that, the testosterone coming in through the blood has to be high enough to act as the raw material that the tissues are now missing. The blood number goes up. That is expected. That is the dose doing its job.
Then Where Did the “55 ng/dL Upper Limit” Come From?
This is one of the most important things a woman should understand before her next lab review.
When your lab report says the female upper limit for testosterone is 55 ng/dL (LabCorp premenopausal) or 45 ng/dL (Quest, age 18+), that number is nota treatment safety threshold [8, 9]. It is not based on outcomes data. It is not from a study showing that women above 55 ng/dL have more breast cancer, more heart disease, or more anything.
It is a statistical range — the upper end of what is found in a population of women not on treatment, run through a particular lab’s particular assay [8, 9, 10]. In other words, the reference range merely tells you the range of serum (blood levels) for the women who had their testosterone levels tested at that lab. That’s it. It doesn’t tell you anything else, and it certainly doesn’t tell you whether those same women had enough testosterone inside all of the cells throughout their bodies.
Two important facts you may not have heard:
Different labs report different “normal” ranges. LabCorp lists adult premenopausal women at 10–55 ng/dL and postmenopausal women at 7–40 ng/dL [8]. Quest lists women 18 and older at 2–45 ng/dL [9]. Endotext, a clinical reference, states plainly that “age-dependent reference ranges are method-specific, and no generalizable cut-point for the diagnosis of testosterone deficiency seems possible” [10].
The assays themselves are unreliable in the female range. A 2019 review in Maturitas states that “most of the available immunoassays lack the required accuracy when dealing with T concentrations… across the entire range for females” [11]. A 2008 review put it the same way: assay quality is a major problem for clinical decision-making in women [12].
So when a clinician says, “Your testosterone is above the upper limit, we need to lower the dose,” what they are actually saying is: “Your number is above the top end of a population range from a particular lab, measured with an assay that is not very accurate in women, that was never built to guide treatment.”
That is not the same thing as “your dose is unsafe.”
What the Major Guidelines Actually Say
This is where it gets interesting. Even the conventional guidelines — the ones often used to argue against Dr. Glaser’s approach — do not say that a blood number alone proves a woman is over-treated. (We’ll talk about the shortcomings of so-called medical guidelines another day). But suffice it to say that none of the medical guidelines or position statements provide a “normal” blood(serum) testosterone level for women.
The 2019 Global Consensus Position Statement on Testosterone Therapy for Women (signed by the International Menopause Society, the Endocrine Society, NAMS, and others) states there is no validated blood-level cutoff that defines “androgen deficiency” in women [13].
The ISSWSH Clinical Practice Guideline says explicitly: “A total testosterone level should not be used to diagnose HSDD” (the FDA-recognized low-libido condition) [14]. They recommend using it as a baseline for monitoring, not as a diagnostic threshold.
In other words, the same guidelines often used to limit a woman’s dose do not actually claim the blood number tells you whether she has enough testosterone where it matters.
So, where does that leave us?
The honest answer is the one most women are never given.
There is no agreed-upon “right” blood testosterone level for a woman. Not in health. Not in treatment. The major societies all acknowledge this [3, 10, 11, 12, 13, 14].
The blood test reflects only a fraction of total androgen activity in a woman’s body — roughly 10 to 20% of the bioactive androgen story, with the rest happening inside the cells where the blood test cannot see [1, 2, 3].
The “upper limit” on your lab slip is a population statistic from one assay, not a safety ceiling derived from outcomes. Different labs give different numbers. The assays are not accurate in the female range to begin with [8, 9, 10, 11, 12].
This does not mean blood testing is useless. It is useful as a baseline for tracking trends over time and identifying true outliers. It is not a target. It is one piece of information.
The better question is not “Is my number in range?” but “What is my body telling me, and what does my whole picture look like?” That is the question Dr. Glaser, Dr. Labrie, and the consensus guidelines all point toward, even when they disagree about doses [3, 13, 14].
What to Take to Your Clinician
If you are in a conversation about whether your testosterone dose is “too high” based on a blood number, here are reasonable questions to ask:
Which assay did this lab use? How accurate is it for women?
Is this upper limit from outcomes data, or is it a population statistic?
Is my dose being judged by my number, or by how I feel and what is happening in my body?
What does the 2019 Global Consensus Statement actually say about dosing?
Have you read Dr. Glaser’s published work on tissue-level versus serum-level androgens?
You are allowed to ask questions. I recommend that you bring the research with you. You can decide, together, what makes sense for your body.
And if your provider is not “in the know” and unwilling to listen to you or to dose based on symptoms, it’s perfectly reasonable to find a new provider.
Disclaimer: This article is for educational and informational purposes only and is not intended to replace personalized medical advice or individualized care. It is meant to help you understand your physiology, explore evidence-based options, and make informed choices about your health and wellness. Healthcare should be a partnership, not a permission slip, and proactive care is just as essential as treatment. Use this information to engage in open, collaborative discussions with your provider or to make empowered decisions that align with your own values, goals, and comfort level. You are the ultimate authority on your body.
References
[1] Labrie, F., et al. (2017). Androgens in women are essentially made from DHEA in each peripheral tissue according to intracrinology. Journal of Steroid Biochemistry and Molecular Biology, 168, 9–18. https://doi.org/10.1016/j.jsbmb.2016.12.007
[2] Labrie, F. (2019). Intracrinology and menopause: the science describing the cell-specific intracellular formation of estrogens and androgens from DHEA and their strictly local action and inactivation in peripheral tissues. Menopause, 26(2), 220–224. https://doi.org/10.1097/GME.0000000000001177
[3] Glaser, R. (2026). Intracrinology and testosterone pellet therapy: an enzyme-aware, symptom-driven approach to hormone optimization in aging. Cureus, 18(4), e106377. https://doi.org/10.7759/cureus.106377
[4] Burger, H. G. (2002). Androgen production in women. Fertility and Sterility, 77(Suppl 4), S3–S5. https://doi.org/10.1016/S0015-0282(02)02985-0
[5] Davison, S. L., et al. (2005). Androgen levels in adult females: changes with age, menopause, and oophorectomy. Journal of Clinical Endocrinology and Metabolism, 90(7), 3847–3853. https://doi.org/10.1210/jc.2005-0212
[6] Labrie, F., et al. (1997). Marked decline in serum concentrations of adrenal C19 sex steroid precursors and conjugated androgen metabolites during aging. Journal of Clinical Endocrinology and Metabolism, 82(8), 2396–2402. https://doi.org/10.1210/jcem.82.8.4160
[7] Glaser, R., & Dimitrakakis, C. (2013). Reduced breast cancer incidence in women treated with subcutaneous testosterone, or testosterone with anastrozole: a prospective, observational study. Maturitas, 76(4), 342–349. https://doi.org/10.1016/j.maturitas.2013.08.002
[8] Labcorp. (2024). Testosterone, Total, Women, Children, and Hypogonadal Males, LC/MS-MS (test 070001) — reference intervals. Retrieved from https://www.labcorp.com/tests/related-documents/L9688
[9] Quest Diagnostics. (2026). Testosterone, Total, MS (test 15983) — reference ranges. Retrieved from https://testdirectory.questdiagnostics.com/test/test-detail/15983/testosterone-total-ms
[10] Winters, S. J. (2020). Laboratory assessment of testicular function. In K. R. Feingold, B. Anawalt, M. R. Blackman, A. Boyce, G. Chrousos, E. Corpas, W. W. de Herder, K. Dhatariya, K. Dungan, J. Hofland, S. Kalra, G. Kaltsas, N. Kapoor, C. Koch, P. Kopp, M. Korbonits, C. S. Kovacs, W. Kuohung, B. Laferrère, M. Levy, … D. P. Wilson (Eds.), Endotext. MDText.com, Inc. https://www.ncbi.nlm.nih.gov/books/NBK279145/
[11] Kanakis, G. A., et al. (2019). Measuring testosterone in women and men. Maturitas, 125, 41–44. https://doi.org/10.1016/j.maturitas.2019.04.203
[12] Bhasin, et al. (2008). The impact of assay quality and reference ranges on clinical decision making in the diagnosis of androgen disorders. Steroids, 73(13), 1311–1317. https://doi.org/10.1016/j.steroids.2008.07.003
[13] Davis, S. R., et al. (2019). Global Consensus Position Statement on the Use of Testosterone Therapy for Women. Journal of Clinical Endocrinology and Metabolism, 104(10), 4660–4666. https://doi.org/10.1210/jc.2019-01603
[14] Parish, S. J., et al. (2021). International Society for the Study of Women’s Sexual Health Clinical Practice Guideline for the use of systemic testosterone for hypoactive sexual desire disorder in women. Journal of Women’s Health, 30(4), 474–491. https://doi.org/10.1089/jwh.2021.29037