
Duavee Mania: Is It Really Better Than What Is Already in Front of Us?

By: Jill Chmielewski, May 17, 2026
If you have spent any time in the menopause corner of the internet, you have probably heard it by now. Several well-known voices on social media and popular podcasts are promoting the use of Duavee for women to prevent breast cancer, for women with DCIS, or for women who simply want to stay "safe." And just like that, a quiet little pill becomes the next thing every woman is told she should be on to prevent breast cancer.
This piece is not here to talk you out of Duavee. It is here to slow things down. I want to walk through what the PROMISE study actually showed, what it did not show, and what the other option in front of us, testosterone, looks like when you put the two side by side. By the end, my hope is that you can make an informed decision based on the data, not the buzz.
What Is DCIS?
DCIS stands for ductal carcinoma in situ. It means there are abnormal cells inside the milk ducts of the breast, but they have not spread beyond those ducts. Some doctors call it "stage 0 breast cancer." Others call it a "pre-cancer." About 60,000 women in the United States are told they have DCIS every year [1].
What Duavee Actually Is
Duavee is a combination pill. It contains two things:
Conjugated estrogens (CE) — a form of estrogen
Bazedoxifene (BZA) — a SERM, or selective estrogen receptor modulator, that blocks estrogen in some tissues (like the breast and uterus) and lets it through in others (like bone)
Think of bazedoxifene as a traffic cop for estrogen. In the breast, it holds up a stop sign. In the bones, it waves estrogen through.
Duavee was approved by the FDA in 2013 for hot flashes and osteoporosis prevention in postmenopausal women with a uterus [2]. That is its approved use. It is not FDA-approved for breast cancer prevention. Not in healthy women. Not in high-risk women. Not in previvors. Not in women with DCIS.
The Horse Estrogen Question
The "conjugated estrogens" in Duavee come from the urine of pregnant horses. This is the same source as Premarin, a drug that has been controversial for decades [3]. Here is what the production process involves for those animals:
Mares are kept pregnant almost continuously and confined to stalls so small they cannot turn around
They wear rubber urine-collection bags that cause chafing and open sores
Their water is restricted to make the urine more estrogen-concentrated
Their foals are taken within days of birth, and most are slaughtered as industry byproducts
The mares continue in this cycle until they are worn out, then auctioned for slaughter
Estradiol is the main estrogen the human body makes. It is bioidentical, meaning identical in structure to what your own ovaries produce. It can be made from plant sources (soy and wild yam). It is FDA-approved in patch, gel, spray, and pill forms. It is widely available and relatively inexpensive.
Many women have no idea their hormone prescription may be tied to this practice. They may reasonably prefer a bioidentical, cruelty-free option.
The PROMISE Study: What It Actually Showed
Researchers at 10 hospitals across the U.S. ran a study called the PROMISE trial [4]. Women who had just been diagnosed with DCIS were enrolled before their surgery. Researchers had a rare window to test a drug in real breast tissue before that tissue was removed.
Half of the women took Duavee for about four weeks before surgery. The other half took a placebo (a sugar pill). After surgery, the team compared tissue samples. 141 women took part. The study was led by Dr. Swati Kulkarni, a breast surgeon at Northwestern University [5].
What They Measured: Ki-67
The main thing researchers measured was a marker called Ki-67. The simple way to think about it: Ki-67 is a flag a cell raises when it is dividing (when it is making copies of itself) [6].
High Ki-67 = many cells dividing = fast-growing tissue
Low Ki-67 = fewer cells dividing = quieter, more controlled tissue
A lower Ki-67 score is generally a good sign.
Why Ki-67 Can Drop on Its Own
This part is important before you read the results. Ki-67 can fall for many reasons that have nothing to do with the drug being tested. A DCIS diagnosis is often a major wake-up call. Many women immediately:
Cut back on alcohol or stop drinking
Eat better — more vegetables, less sugar and processed food
Start exercising regularly
Lose weight, which lowers inflammatory signals
Sleep better and reduce stress
All of these can lower Ki-67 on their own. Researchers call this the "diagnosis effect."
In PROMISE, even women on the sugar pill saw Ki-67 drop by about 1 point. This is the diagnosis effect at work. Women who took Duavee saw it drop by about 5.62 points. The difference was statistically significant (p = 0.016) [4]. That difference is real and worth noting.
But Ki-67 is a tissue marker. It does not mean that "cancer has been prevented." It is simply a surrogate marker.
What "Surrogate Endpoint" Actually Means
When a study measures Ki-67 instead of breast cancer, it is using a shortcut. The hope is that the shortcut tracks closely enough with the real outcome that you can trust it. Sometimes it does. Often it does not.
The history of women's health is full of medications that looked great on surrogate endpoints and then failed, or caused harm, when researchers finally measured the outcome that actually mattered [7].
A drop in Ki-67 does not translate to "it prevented breast cancer." It is a hopeful signal, but not proof.
The Limits of the PROMISE Study (Please Read This)
It was a four-week study. Long enough to see a tissue marker change. Not long enough to know if women will go on to develop invasive breast cancer.
Ki-67 is not a cancer outcome. The FDA does not accept Ki-67 reduction as proof that a drug prevents cancer. Long-term trials measuring real cancer rates are what is needed.
Only 94 of 141 women had usable Ki-67 data, about 67% of those enrolled.
This was a Phase 2 trial. Phase 2 trials check whether a treatment might work. Phase 3 trials, which are larger and longer and measure real outcomes like cancer incidence, are what is needed before any new FDA approval.
No comparison to standard treatments. The study compared Duavee to a sugar pill, not to tamoxifen, not to an aromatase inhibitor, not to anything currently used.
Not yet peer-reviewed. The data were presented at a medical conference. The full paper has not yet been reviewed and published in a scientific journal [8].
The horse estrogen question. We do not know if the same results would appear with bioidentical estradiol. This is an unstudied variable.
Bazedoxifene has its own side effects. In Phase 3 safety trials, women on bazedoxifene reported leg cramps, joint pain, back pain, muscle spasms, neck pain, nausea, and dizziness [9]. Bazedoxifene, like all SERMs, also raises the risk of blood clots, deep vein thrombosis and pulmonary embolism, similar to other drugs in its class [9].
No fracture outcome data. Bazedoxifene improves bone density on a scan. It has not yet been shown in long-term trials to reduce actual fractures [2]. We have the surrogate. We do not have the outcome that matters.
Out of 100 Women Taking Duavee, How Many Avoid Breast Cancer?
We do not know. That number does not exist. No one has measured it. For Duavee, that row of the table is empty. Anyone who tells you Duavee will prevent your breast cancer is making a guess. An educated guess, maybe. But a guess.
A Critical Question: Can Blocking Estrogen Backfire?
This is something most mainstream coverage of PROMISE will not raise. But it is a legitimate scientific concern.
When breast cancer cells are exposed to drugs that block estrogen over time, some of them can develop a mutation in a gene called ESR1. This is the gene that makes the estrogen receptor.
An ESR1 mutation changes the shape of the receptor so it gets stuck in the "on" position. It keeps telling the cell to grow even when there is no estrogen present and even when the woman is taking a drug to block estrogen in that tissue [10].
This is called endocrine resistance. It is one of the biggest challenges in treating ER-positive breast cancer.
ESR1 mutations are very rare when breast cancer is first found, about 1 out of 100 cases. After being on an aromatase inhibitor or tamoxifen for a period of time, these mutations show up in about 1 to 4 out of 10 women whose cancer has spread. They can make the cancer much harder to treat [10].
PROMISE ran for only four weeks, which is far too short for endocrine resistance to develop. But if Duavee were ever used long-term in DCIS women as a risk-reduction strategy, which is exactly what is being floated, this would be an important question to answer.
No one is saying Duavee causes ESR1 mutations. We simply do not know. And in a setting where many oncologists recommend long-term hormone suppression for years, it is a question worth asking.
The Patent Problem
Duavee is a patented drug made by Pfizer. The main active U.S. patent is expected to expire around March 2027. After that, generics could enter the market [11].
To obtain new FDA approval for DCIS, Pfizer would need to fund a large Phase 3 trial, costing tens of millions of dollars and running for years. But that investment only pays off if the patent window gives them years of profit after approval.
The PROMISE trial itself was funded by the National Cancer Institute, a public grant, not Pfizer. That lends independence to the findings. But a Phase 3 trial would ultimately require industry involvement.
A drug about to go generic is not an attractive investment target. As the patent window closes, so does the commercial incentive to generate the definitive evidence women with DCIS deserve.
Testosterone: The Option Already in Front of Us
This is the section most breast cancer articles never get to. But the data deserves attention, and a fair comparison.
What Testosterone Does for the Whole Body
Before we get to the breast cancer data, it is worth saying what testosterone actually does for women. This is where the drug industry's focus on SERMs and aromatase inhibitors misses the bigger picture.
When testosterone levels are restored in women, the benefits span the entire musculoskeletal system and beyond [12]:
Bones. Testosterone supports bone mineral density directly through the androgen receptor in bone cells. And unlike bazedoxifene, which improves bone density markers but has no fracture outcome data yet, testosterone also builds the muscle strength needed to prevent the falls that cause fractures. Real fracture protection is bone strength plus the muscle to stay upright.
Muscle. Testosterone helps women maintain lean muscle mass. When testosterone falls, muscle loss speeds up. This is called sarcopenia. Restoring testosterone preserves strength, improves body composition, and makes daily activities safer with age.
Collagen. Collagen is the protein that holds skin, joints, tendons, and bones together. Research shows women treated with estradiol and testosterone together had about 48% greater collagen content in skin compared to untreated women over the same period [13]. This is not just about appearance. Collagen is the framework of your joints and connective tissue throughout your body.
Stamina and energy. Restoring testosterone to healthy levels improves energy, exercise endurance, and overall stamina.
Mood and motivation. Testosterone supports dopamine pathways in the brain. Low testosterone in women is linked to flat mood, low motivation, poor concentration, and what many describe as brain fog. Restoring it can improve focus, drive, and emotional resilience.
Why Testosterone Matters in Breast Cancer Specifically
A landmark 2021 study in Nature Medicine found that the androgen receptor (AR), the receptor that testosterone binds to, acts as a tumor suppressor in ER-positive breast cancer [14].
In plain terms: when testosterone connects to the AR, it appears to put the brakes on ER-positive cancer cell growth. It does not feed cancer. It suppresses it.
Most ER+ breast cancers also express AR [15]. That means most women with the kind of DCIS studied in PROMISE also carry this testosterone receptor, a protective target that mainstream oncology largely ignores.
When an aromatase inhibitor is added alongside testosterone, it prevents the testosterone from converting to estrogen. That keeps the balance shifted toward AR-mediated effects in the breast.
The Wider Body of Evidence
You are not going to find a single, large, randomized, placebo-controlled trial with breast cancer incidence as the primary endpoint for testosterone in women. That trial does not exist. It is not going to exist. The reasons are simple: testosterone has been off-patent since 1937, no drug company can recover the cost of running it, and the public funding agencies that could fund it have not.
That is the world we are working in. So when randomized trials are not coming, the responsible move is not to throw up our hands. It is to use what we have — real-world evidence, clinical cohort data, primate biology, and the physiology of the androgen receptor itself, and ask whether the signals all point in the same direction. With testosterone and the breast, they do.
What "Real-World Evidence" Actually Means
Real-world evidence is data collected from clinical practice rather than from controlled experiments. It includes prospective cohort studies, clinical registries, electronic health records, insurance databases, and pathology archives. The FDA itself now formally uses real-world evidence to support drug approvals when randomized trials are not feasible or ethical [16].
Real-world evidence cannot prove cause and effect the way a randomized trial can. But when the signal is consistent across many independent cohorts, across different decades, across different countries, across different research groups, that consistency is its own kind of evidence. It is the kind of evidence we use for things like long-term medication monitoring and for studying anything that cannot ethically be randomized.
For testosterone and the breast, the real-world evidence is now extensive enough to take seriously.
The Dimitrakakis 2004 Cohort
Before Dr. Glaser even began her Dayton study, Dr. Constantine Dimitrakakis (now her longtime collaborator) published a cohort study in Menopause in 2004 [17]. He followed 508 postmenopausal women who took testosterone added to their usual estrogen-progestin therapy. He compared their breast cancer rates to women on estrogen-progestin alone.
Women on the testosterone-containing regimen had a breast cancer rate of about 293 per 100,000 woman-years. Women on standard estrogen-progestin had a rate of about 380 per 100,000. The general female population had a rate of about 350 per 100,000 [17].
In plain English: adding testosterone to standard hormone therapy was linked to lower breast cancer rates, not higher. This was twenty years ago. The data has continued to point that direction ever since.
The 15-Year Dayton Cohort
Dr. Rebecca Glaser is a breast surgeon at Wright State University in Dayton, Ohio. She has studied subcutaneous testosterone implants, small pellets placed under the skin that slowly release testosterone, for more than 15 years [18].
She has followed 1,267 women in Dayton since 2008. These women received testosterone pellets for hormone deficiency symptoms, not for cancer prevention. Their breast cancer rates were then compared to what would be expected for women their age based on the national SEER database (a large U.S. government cancer registry) [18].
At 15 years: 166 fewer invasive breast cancers per 100,000 women per year compared to what the national data would predict. Statistically significant (p = 0.008). The result has held up and grown stronger over 15 years of follow-up [18].
When women stopped testosterone therapy for more than 240 days, their cancer risk drifted back toward the national average. The protection appears to require ongoing therapy.
Dr. Glaser has also published case reports of women with ER-positive invasive breast cancer who received testosterone implants combined with aromatase inhibitors before surgery, showing measurable tumor shrinkage [19].
The Ribeiro 2025 Meta-Analysis
This is the most important new piece of evidence, and it has not received the attention it deserves.
In July 2025, Ribeiro and colleagues published a systematic review and meta-analysis at the Endocrine Society meeting [20]. They pooled data from multiple studies covering 5,747 postmenopausal women receiving testosterone therapy. Follow-up ranged from 4.4 to 10 years. They compared breast cancer rates in these women to population-based controls.
The pooled result: a statistically significant reduction in breast cancer incidence in women on testosterone (p = 0.02) [20].
Out of 5,747 women followed for years, across many independent studies, by many independent research groups, testosterone was linked to fewer breast cancers, not more.
What Happens in the Breasts of Transgender Men
There is one more piece of real-world evidence that does not get talked about in women's health circles. It is some of the most direct evidence we have about what testosterone does to breast tissue in a living human body over time.
Transgender men, people assigned female at birth who take testosterone for years before undergoing gender-affirming chest surgery, provide pathologists with a unique window into what high-dose testosterone does to breast tissue. Their breast tissue is removed at surgery and examined under the microscope.
What pathologists find, across many independent studies, is remarkably consistent [21, 22]:
Lobular atrophy — the glandular tissue most linked to breast cancer development shrinks
Lower lobular density — fewer of the structures from which breast cancers arise
Higher proportion of fibrous tissue — the protective stromal background expands
Lower rates of atypia — the precancerous changes that worry pathologists are rarer than in cisgender women's breast tissue
Lower rates of cysts, apocrine metaplasia, calcifications, and columnar cell changes — all markers of mild proliferative activity
Longer testosterone exposure was linked to more pronounced effects — a dose-response relationship that strengthens the biological argument
A 2023 systematic review of 76 studies on testosterone exposure and breast cancer risk in transmasculine individuals concluded that breast cancer incidence in this population is lower than in cisgender women, and that the histology shows testosterone is doing something protective to glandular tissue [23].
These are people taking testosterone at higher doses than women on physiologic replacement, for years, with their breast tissue intact. If testosterone were going to feed breast cancer, this is the population that would show it. They do not.
Primate Biology: What the Tissue Actually Does
The cohort data is consistent. The transgender data is consistent. And the laboratory biology explains why.
In 2000, Dr. Carolyn Bondy's team at the NIH ran a classic study in ovariectomized rhesus monkeys (whose breast tissue is the closest non-human model to women's) [24]. They treated the animals with placebo, estradiol alone, estradiol plus progesterone, estradiol plus testosterone, or tamoxifen. They then measured what happened to mammary epithelial cells, the cells that line the milk ducts and give rise to most breast cancers.
The findings were striking:
Estradiol alone increased mammary cell proliferation about sixfold
Adding progesterone did not change estrogen's proliferative effect
Adding testosterone reduced estrogen-driven proliferation by about 40%, and entirely shut down the estrogen-driven rise in estrogen receptor expression
Tamoxifen unexpectedly also increased proliferation in this model (about three-fold), though it reduced estrogen receptor expression below baseline
Translation: testosterone, added to estrogen, puts the brakes on the very process, epithelial cell proliferation, that breast cancers are thought to arise from.
The same group followed up in 2003 with a paper directly titled "A physiologic role for testosterone in limiting estrogenic stimulation of the breast" [25]. The argument is right there in the title. Testosterone is not opposing estrogen because it is a "male hormone fighting a female one." It is opposing estrogen because the breast tissue has both estrogen receptors and androgen receptors, and the two systems are designed to balance each other out.
Putting It All Together
Step back and look at what we have, gathered from completely independent sources over more than two decades:
Dimitrakakis 2004 — 508 women, lower breast cancer rates with testosterone added to standard hormone therapy
Glaser 2013, 2019, 2025 — 1,267 women followed up to 15 years in Ohio, statistically significant reduction in invasive breast cancer
Ribeiro 2025 meta-analysis — 5,747 postmenopausal women pooled, statistically significant reduction (p = 0.02)
Transgender pathology studies — breast tissue shows lobular atrophy and reduced precancerous changes after years of testosterone exposure
Primate studies — testosterone reduces estrogen-driven breast cell proliferation by 40%
Nature Medicine 2021 — androgen receptor is a tumor suppressor in ER-positive breast cancer
Every line of evidence points the same direction. That is rare. In medicine, when cohort data, pathology data, animal data, and molecular biology all agree, that is usually the moment the field starts taking a question seriously.
For testosterone, the field has not. Not because the data is wrong. Because no drug company can profit from confirming it.
What "We Don't Have an RCT" Really Means
When a clinician tells you, "There is no randomized trial proving testosterone prevents breast cancer," that statement is technically true. It is also incomplete.
A randomized trial is one form of evidence. It is one of the most rigorous forms when the question is whether a single intervention causes a single outcome. But it is not the only form. It cannot ask every question that matters.
The FDA's own guidance on real-world evidence acknowledges this directly [16]. The question is not "do we have an RCT?" The question is: when we look at all the available evidence — cohort, registry, pathology, animal, and molecular — does the signal converge? For testosterone and the breast, it does. Across decades, across countries, across research groups, across study designs, across species.
Two Drugs, One Structural Problem
Step back and notice the pattern.
Duavee has a four-week, 141-woman Phase 2 trial measuring a tissue marker. Its patent expires in 2027, so a Phase 3 trial is unlikely. The drug company has no real incentive to prove it works for breast cancer prevention before the patent runs out.
Testosterone has nearly 8,000 women's worth of consistent observational data across multiple independent research groups and three continents, plus primate biology and transgender pathology all pointing the same direction. It has been off-patent since 1937. No drug company has any incentive to fund the Phase 3 trial that would settle the question.
Both have biological rationale. Both have early clinical signals. Neither has a definitive Phase 3 trial. Both face the same obstacle: the economics of drug development do not reward research into unpatentable or nearly-expired treatments.
Duavee is getting the podcast moment. Testosterone is getting silence. Neither is getting the trial it deserves.
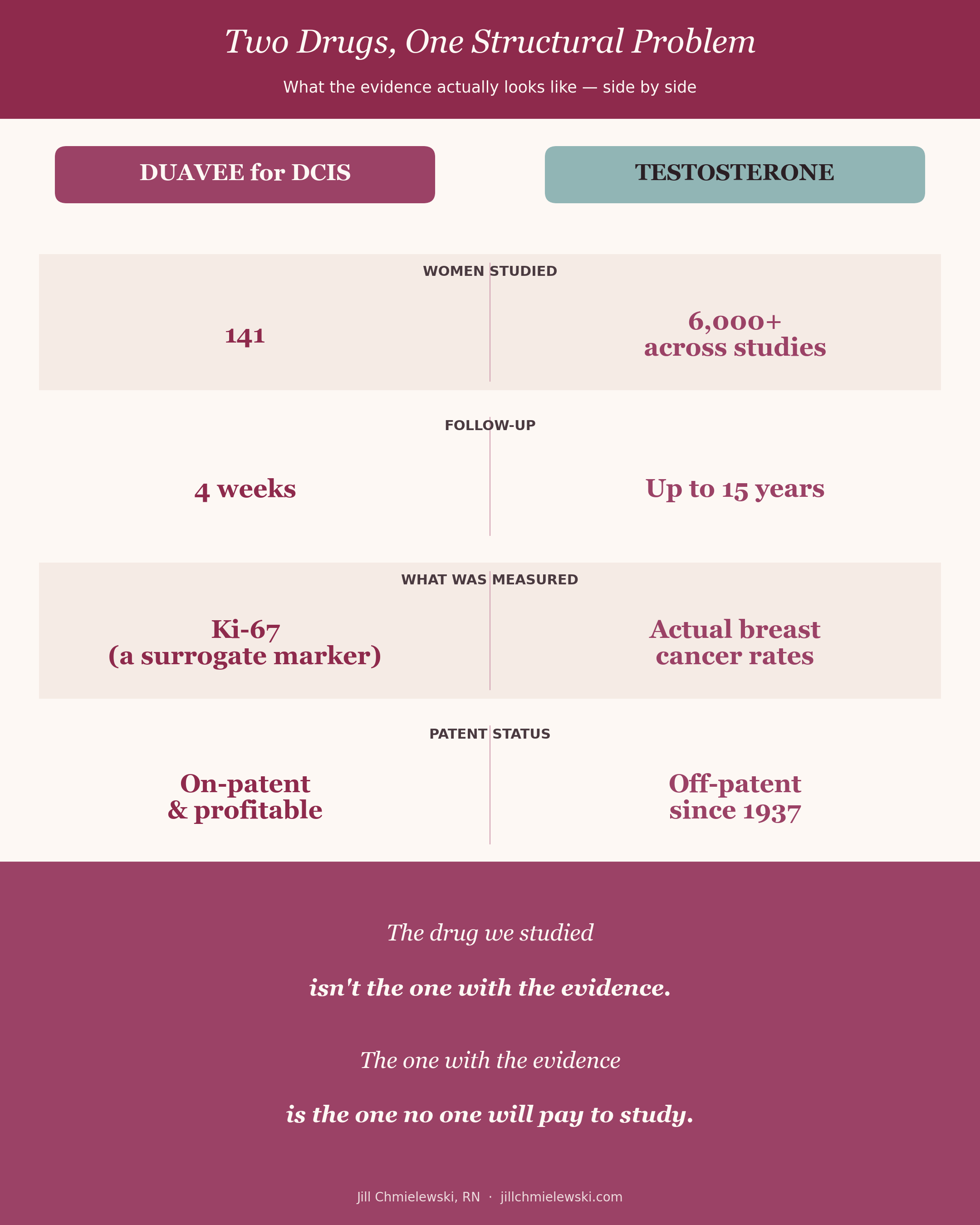
Side by side comparison of Duavee and Testosterone.
What This Means for You
If you have DCIS, are dealing with hot flashes or sleep problems, or are simply trying to figure out the best path forward, here is where things stand.
The PROMISE data are interesting. Duavee appears to reduce breast cell activity over four weeks and improves hot flashes. That is a real finding worth discussing with your team.
But the evidence has real limits. Four weeks. One tissue marker. Phase 2. Horse-derived estrogens. No peer-reviewed paper yet. No comparison to existing treatments. No long-term safety data in healthy or high-risk women. No fracture data. No survival data.
Ask about testosterone. The data are not from a Phase 3 trial. But the biological rationale is strong, the observational evidence is consistent across decades and continents, and the benefits span the entire body in ways no SERM can match.
Ask about ESR1. If a clinician recommends long-term estrogen blockade — Duavee, tamoxifen, or an aromatase inhibitor, ask what the plan is if resistance develops. This is a reasonable and clinically important question.
Ask for a real benefits-vs-risks conversation for each option. You deserve individualized care based on your tumor biology, your symptoms, your quality of life, and your priorities — not based on what is loudest in the algorithm this week.
Bottom Line
The PROMISE study is the first randomized trial to show that a menopause drug can reduce breast tissue activity in ER+ DCIS while relieving hot flashes. That is a meaningful step.
But the drug uses horse-derived estrogens when bioidentical estradiol exists. Its side effects include joint pain, leg cramps, and clot risk. We have no fracture data. We have no long-term data on cancer incidence. And the patent expires in 2027, making a definitive Phase 3 trial unlikely.
Meanwhile, decades of data on testosterone, across nearly 8,000 women, primate biology, transgender pathology, and the molecular biology of the androgen receptor itself, show a measurable reduction in invasive breast cancer, with absolute benefits across bone, muscle, collagen, energy, and mood. And no commercial sponsor is willing to fund the trial that could confirm it.
Women with DCIS, and women trying to prevent breast cancer, have been told "no" for too long. The biology says the answer is far more nuanced. Find a clinician who will look at all of it with you.
For more information about breast cancer, see my other articles and resources:
Hormones & Breast Cancer: What’s Fact, What’s Fiction?
The History of Breast Cancer Treatments and the Misguided War on Estrogen
The Truth About Estrogen, Breast Cancer, and Hormone Therapy: What the Latest Research Reveals
Check out the Breast Cancer Series in the Balance App
References
1] Breast Cancer Research Foundation. (2024). About DCIS (ductal carcinoma in situ). https://www.bcrf.org/about-breast-cancer/dcis-ductal-carcinoma-in-situ/
[2] U.S. Food and Drug Administration. (2024). Duavee (conjugated estrogens/bazedoxifene) prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/022247s010lbl.pdf
[3] People for the Ethical Treatment of Animals. (2024). Hormone replacement therapy: The tragedy of Premarin. https://www.peta.org/issues/animals-used-for-experimentation/premarin-hormone-replacement-therapy/
[4] Kulkarni, S., et al. (2025). The PROMISE Study: CE/BZA vs placebo in postmenopausal women with DCIS. ASCO Annual Meeting 2025, Abstract 512. https://ascopubs.org/doi/10.1200/JCO.2025.43.16_suppl.512
[5] ecancer Medical Science. (2025). ASCO 2025: Menopause drug Duavee may help prevent invasive breast cancer. https://ecancer.org/en/news/26527-asco-2025-menopause-drug-duavee-may-help-prevent-invasive-breast-cancer
[6] Davey, M. G., et al. (2021). Ki-67 as a prognostic biomarker in invasive breast cancer. Cancers, 13(17), 4455. https://doi.org/10.3390/cancers13174455
[7] Chlebowski, R. T., et al. (2020). Association of menopausal hormone therapy with breast cancer incidence and mortality during long-term follow-up of the Women's Health Initiative randomized clinical trials. JAMA, 324(4), 369–380. https://doi.org/10.1001/jama.2020.9482
[8] Teplinsky, E. (2025). ASCO 2025 updates in early stage breast cancer. https://drteplinsky.substack.com/p/asco-2025-updates-in-early-stage
[9] Christiansen, C., et al. (2010). Safety of bazedoxifene in a randomized, double-blind, placebo- and active-controlled phase 3 study of postmenopausal women with osteoporosis. BMC Musculoskeletal Disorders, 11, 130. https://doi.org/10.1186/1471-2474-11-130
[10] Jeselsohn, R., et al. (2015). ESR1 mutations — a mechanism for acquired endocrine resistance in breast cancer. Nature Reviews Clinical Oncology, 12(10), 573–583. https://doi.org/10.1038/nrclinonc.2015.117
[11] Pharsight GreyB. (2024). Duavee drug patent profile — expiration analysis. https://pharsight.greyb.com/drug/duavee-patent-expiration
[12] Rojas-Zambrano, J. G., et al. (2025). Benefits of testosterone hormone in the human body: A systematic review. Cureus, 17(2), e78785. https://doi.org/10.7759/cureus.78785
[13] Brincat, M., et al. — cited in GREM Journal. (2024). Menopause and the effects of hormone replacement therapy on skin aging: A short review. https://gremjournal.com/journal/01-2024/menopause-and-the-effects-of-hormone-replacement-therapy-on-skin-aging-a-short-review/
[14] Hickey, T. E., et al. (2021). The androgen receptor is a tumor suppressor in estrogen receptor-positive breast cancer. Nature Medicine, 27(2), 310–320. https://doi.org/10.1038/s41591-020-01168-7
[15] Ravaioli, S., et al. (2022). Androgen receptor in breast cancer: The "5W" questions. Frontiers in Endocrinology, 13, 977331. https://doi.org/10.3389/fendo.2022.977331
[16] U.S. Food and Drug Administration. (2024). Real-world evidence framework. https://www.fda.gov/science-research/science-and-research-special-topics/real-world-evidence
[17] Dimitrakakis, C., et al. (2004). Breast cancer incidence in postmenopausal women using testosterone in addition to usual hormone therapy. Menopause, 11(5), 531–535. https://doi.org/10.1097/01.GME.0000119983.48235.D3
[18] Glaser, R., et al. (2025). Incidence of invasive breast cancer in women treated with testosterone implants: Dayton prospective cohort study — 15-year update. Advances in Preventive Medicine. https://www.gavinpublishers.com/article/view/incidence-of-invasive-breast-cancer-in-women--treated-with-testosterone-implants-dayton-prospective-cohort-study-15-year-update
[19] Glaser, R. L., & Dimitrakakis, C. (2014). Rapid response of breast cancer to neoadjuvant intramammary testosterone-anastrozole therapy: neoadjuvant hormone therapy in breast cancer. Menopause, 21(6), 673–678. https://doi.org/10.1097/GME.0000000000000096
[20] Ribeiro, S. A. G., et al. (2025). Testosterone therapy and breast cancer risk in postmenopausal women: A systematic review and meta-analysis. Journal of the Endocrine Society, 9(Suppl 1), bvaf149.1989. https://doi.org/10.1210/jendso/bvaf149.1989
[21] Wolters, E. A., et al. (2022). Histopathologic features of breast tissue from transgender men and their associations with androgen therapy. American Journal of Clinical Pathology, 159(1), 43–52. https://doi.org/10.1093/ajcp/aqac123
[22] Chaum, M., et al. (2023). Masculinizing hormone therapy effect on breast tissue: Changes in estrogen and androgen receptors in transgender female-to-male mastectomies. The Breast, 72, 103596. https://doi.org/10.1016/j.breast.2023.103596
[23] Gurrala, R. R., et al. (2023). The impact of exogenous testosterone on breast cancer risk in transmasculine individuals. Annals of Plastic Surgery, 90(1), 96–105. https://doi.org/10.1097/SAP.0000000000003321
[24] Zhou, J., et al. (2000). Testosterone inhibits estrogen-induced mammary epithelial proliferation and suppresses estrogen receptor expression. FASEB Journal, 14(12), 1725–1730. https://doi.org/10.1096/fj.99-0863com
[25] Dimitrakakis, C., et al. (2003). A physiologic role for testosterone in limiting estrogenic stimulation of the breast. Menopause, 10(4), 292–298. https://doi.org/10.1097/01.GME.0000055522.67459.89
Disclaimer: This article is for educational and informational purposes only and is not intended to replace personalized medical advice or individualized care. It is meant to help you understand your physiology, explore evidence-based options, and make informed choices about your health and wellness. Healthcare should be a partnership, not a permission slip, and proactive care is just as essential as treatment. Use this information to engage in open, collaborative discussions with your provider or to make empowered decisions that align with your own values, goals, and comfort level. You are the ultimate authority on your body.